35 year old male with SOB and Pedal edema
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent.
Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs.
This E log book also reflects my patient-centered online learning portfolio and your valuable inputs on the comment box is welcome.
Case presentation:
35 year old male labourer by occupation who is the resident of nalgonda presented with pedal edema since 1 month and sob since yesterday
Patient was apparently asymptomatic 1 month back later he developed pedal edema Which was gradual in onset progressed to knee , associated with facial puffiness then he went to chityala and he has taken the medications which was prescribed by local doctor ,symptoms got relieved.
Then yesterday night he developed pedal edema associated sob which was sudden in onset
No aggrevating and relieving factors
For which his wife fed 1 bread and milk and later he vomited.
No h/o chestpain
No h/o palpitations
Past h/o :
No similar complaints in past
N/k/c/o DM , HTN ,ASTHMA ,CAD, EPILEPSY,TB
Personal h/o :
sleep adequate
Diet mixed
Decreased urine output since morning
Addictions :
Patient started consuming alcohol since 17 yrs ( unadulterated tody and whiskey 180ml once in 15 days gradually increased to 360ml of whiskey in the span of 10 yrs)
From past 5- 6 years he developed binge drinking pattern and would drink on days he had money . He used to drink for 3- 4 days continuously and he don't drink for the next 15 days and his last drink was on 12th oct ( 750ml whiskey)
H/o of tobacco chewing ( 1 packet / day ) since 17 yrs
On examination -
Pt was unresponsive with frothing with spo2 48%
In view of falling saturation , patient was intubated with ET 7 , Inj Midazolam 2cc/w/stat , Inj glycopycolate 2cc/ stat with inj NORAD - DS @6ml/hr
Started on Inj Dobutamine @1ml/hr
No pallor ,
No icterus ,
No cyanosis ,
No clubbing,
Bilateral pitting type of pedal edema is present upto knee
His vitals :
Afebrile to touch
Bp - not recordable ( at 3: 30 am)
Bp at 4:00am - 60/40 mmhg
Pulse - feeble
RR - 30cpm
Spo2 - 48% at room air
GRBS - 148mg%
Systemic :
P/A :
Shape of abdomen : obese
no scars , sinuses ,no distended veins ,hernial orifices free ,soft
No tenderness
RS : BAE + Nvbs heard
No added sounds
CNS : NAD
CVS :
S1 S2 heard
No murmurs
Day1-
Investigations ordered :
Ecg

2d echo

HRCT

HbsAg


Blood c/s


CHEST X RAY :

Treatment given :
HEAD END ELEVATION
OXYGENATION TO MAINTAIN SPO2>90%
Intermittent BIPAP
INJ NORAD - DS ( 2 AMP IN 20 ML NS @0.5 ML/ HR
INJ DOPAMINE 1 AMP IN 20 ML NS @0.5ML /HR
INJ PANTOP 40 MG /IV / OD
INJ PIPTAZ 4.5MG/IV/ STAT
INJ THIAMINE 1 AMP IN 100ML NS/ IV/BD
I/O CHARTING
DAILY WEIGHT MONITORING
BP/ PR HOURLY
Provisional diagnosis on admission:
Acute decompensated heart failure with ischemic hepatits with AKI ( DCMP SECONDARY TO ALCOHOL)
Day 2-
No fresh complaints
SOB - decreased
O/E :
Patient is sedated , pupils : sluggish to light
No signs of icterus ,cyanosis , clubbing
Vitals : afebrile
BP - 80 /40mmhg
PR - 117 bpm
GRBS - 123 mg %
OUTPUT - 75ml
CVS -S1 S2 +
RS - BAE + ,NVBS
P/A - SHAPE OF ABDOMEN - OBESE
CNS - NFND
Investigations
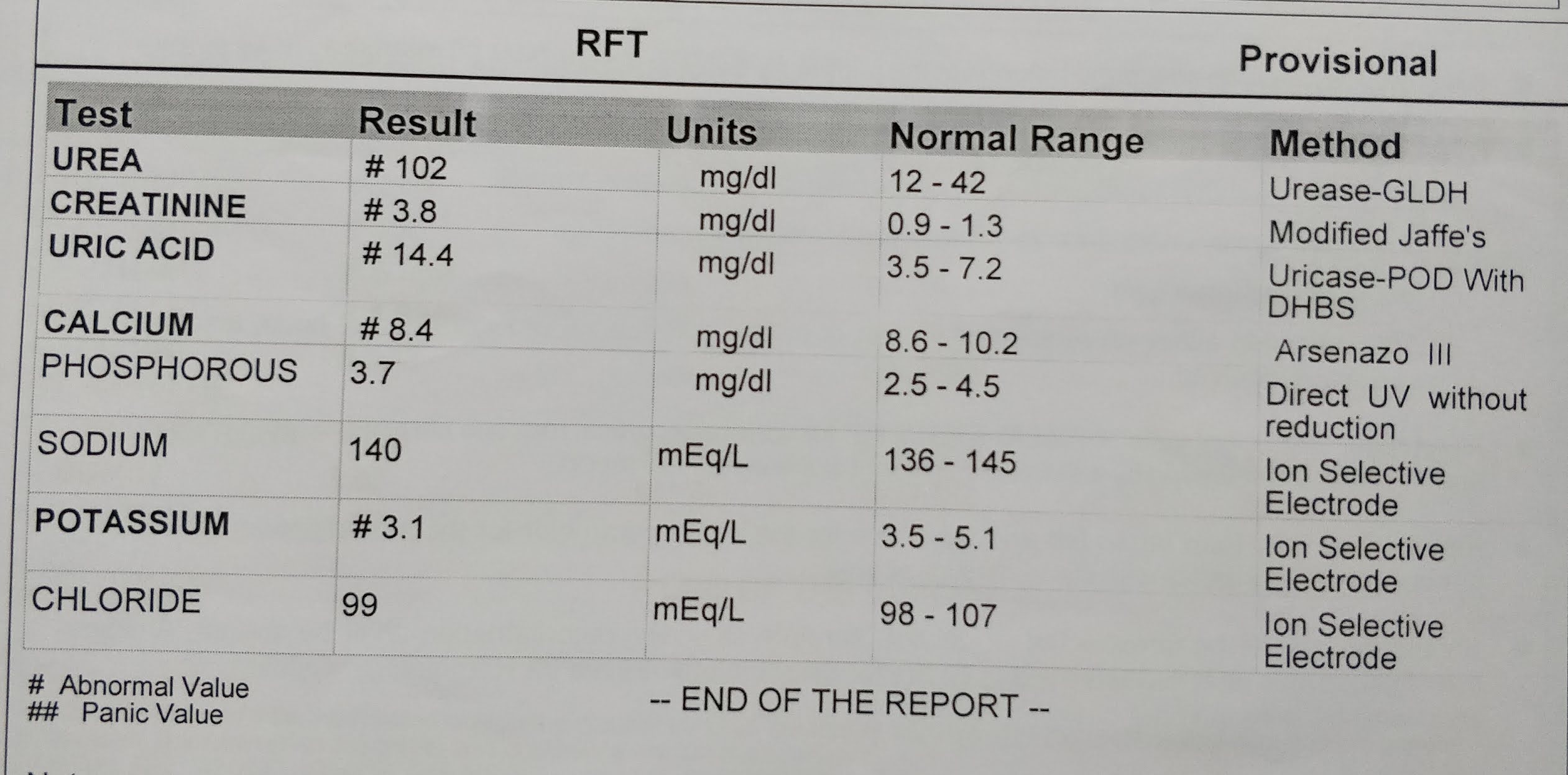
RFT

LFT

Treatment given:
HEAD END ELEVATION
CHANGE POSITION FREQUENTLY
ORAL SUCTION 2ND HOURLY
RT FEEDS ( 2ND HOURLY - 30 ML MILK
HOURLY - 50 ML WATER )
INJ NORAD - DS ( 2 AMP IN 20 ML NS @0.5 ML/ HR
INJ DOPAMINE 1 AMP IN 20 ML NS @0.5ML /HR
INJ PANTOP 40 MG /IV / OD
INJ PIPTAZ 4.5MG/IV/ STAT
INJ THIAMINE 1 AMP IN 100ML NS/ IV/TID
INJ LASIX ( 20 MG/ HR )
IVF - 10MLNS + 10 ML LASIX @ 5 ML/ HR IF SBP > 100MMHG
I/O CHARTING , GRBS 8TH HOURLY
BO/ PR HOURLY /SPO2
Diagnosis- Acute decompensated heart failure with ischemic hepatits with AKI ( DCMP SECONDARY TO ALCOHOL) with ISCHEMIC HEPATITS
WITH AKI
Day 3
No fresh complaints
Pedal edema - decreased
O/E :
Patient is Conscious, coherent
Pupils - NSRL
I/O - 1610/6000ml
Vitals : afebrile
BP - 120/80 mmhg
PR - 92 bpm, normal volume , regular
GRBS - 112mg %
CVS - S1 ,S2 + ,JVP - NORMAL
RS - BAE + ,NVBS
P/A - Obese, soft , non tender.
CNS - NFND
Investigations:
Hemogram

RFT
LFT

CUE

PT

APTT

Treatment given:
HEAD END ELEVATION
RT FEEDS ( 2ND HOURLY - 30 ML MILK , HOURLY - 50 ML WATER )
INJ PANTOP 40 MG /IV / OD
INJ PIPTAZ 2.25MG/IV/QID
INJ THIAMINE 1 AMP IN 100MG / IV/TID
INJ LASIX ( 40 MG/ IV / TID HR ) IF SBP > 100MMHG
TAB AZITHROMYCIN 500MG / OD
NEB WITH MUCOMIST - 6TH HOURLY
BUDECORT - 12TH HOURLY
CHEST PHYSIOTHERAPY FOR 4TH HOURLY
ORAL FLUIDS UPTO 1.5 LIT/DAY
ALLOW SOFT DIET
SYP MUCAINE GEL 15 ML - 15 MIN BEFORE EACH MEAL
INJ HYDROCORTISONE 100MG/ IV / STAT
I/O CHARTING
BO/ PR HOURLY /SPO2
Diagnosis : RIGHT HEART FAILURE WITH PRESERVED EF 58%
WITH BERIBERI (DCMP)?
WITH AKI?
WITH HEPATITS SECONDARY TO ISCHEMIA? ,
WITH MODS?
Day 4( 16/10/20)
No fresh complaints
Pedal edema - decreased
Investigations:
Hemogram

RFT

O/E :
Patient is Conscious.
Vitals:
Febrile - 101F
BP - 120/80 mmhg
PR - 92 bpm, normal volume , regular
CVS - S1 ,S2 + ,JVP - NORMAL
RS - BAE + ,NVBS
P/A - Obese, soft , non tender.
CNS - NFND
Treatment given:
HEAD END ELEVATIOn
INJ PANTOP 40 MG /IV / OD
INJ PIPTAZ 2.25MG/IV/QID
INJ THIAMINE 100MG IN 100ML NS IV/TID
INJ LASIX ( 40 MG/ IV / TID HR ) IF SBP > 100MMHG
TAB AZITHROMYCIN 500MGPO / OD
NEB WITH MUCOMIST - 6TH HOURLY
BUDECORT - 12TH HOURLY
CHEST PHYSIOTHERAPY FOR 4TH HOURLY
ORAL FLUIDS UPTO 1.5 LIT/DAY
ALLOW SOFT DIET
SYP MUCAINE GEL 15 ML - 15 MIN BEFORE EACH MEAL
INJ HEPARIN 5000 / IV / TID
Diagnosis : RIGHT HEART FAILURE WITH PRESERVED EF 58%
WITH BERIBERI (DCMP)?
WITH AKI?
WITH HEPATITS SECONDARY TO ISCHEMIA? ,
WITH MODS?
Day 5 (17/10/20)
No fresh complaints
Pedal edema decreased
Sob decreased








Comments
Post a Comment